
{kind=link}
{kind=link}
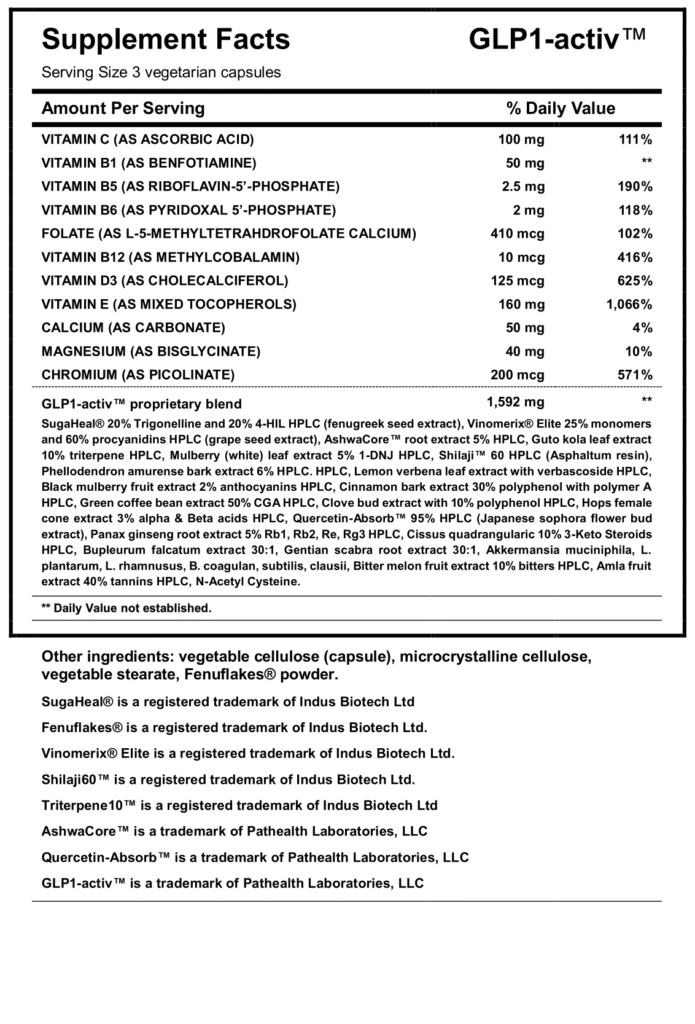
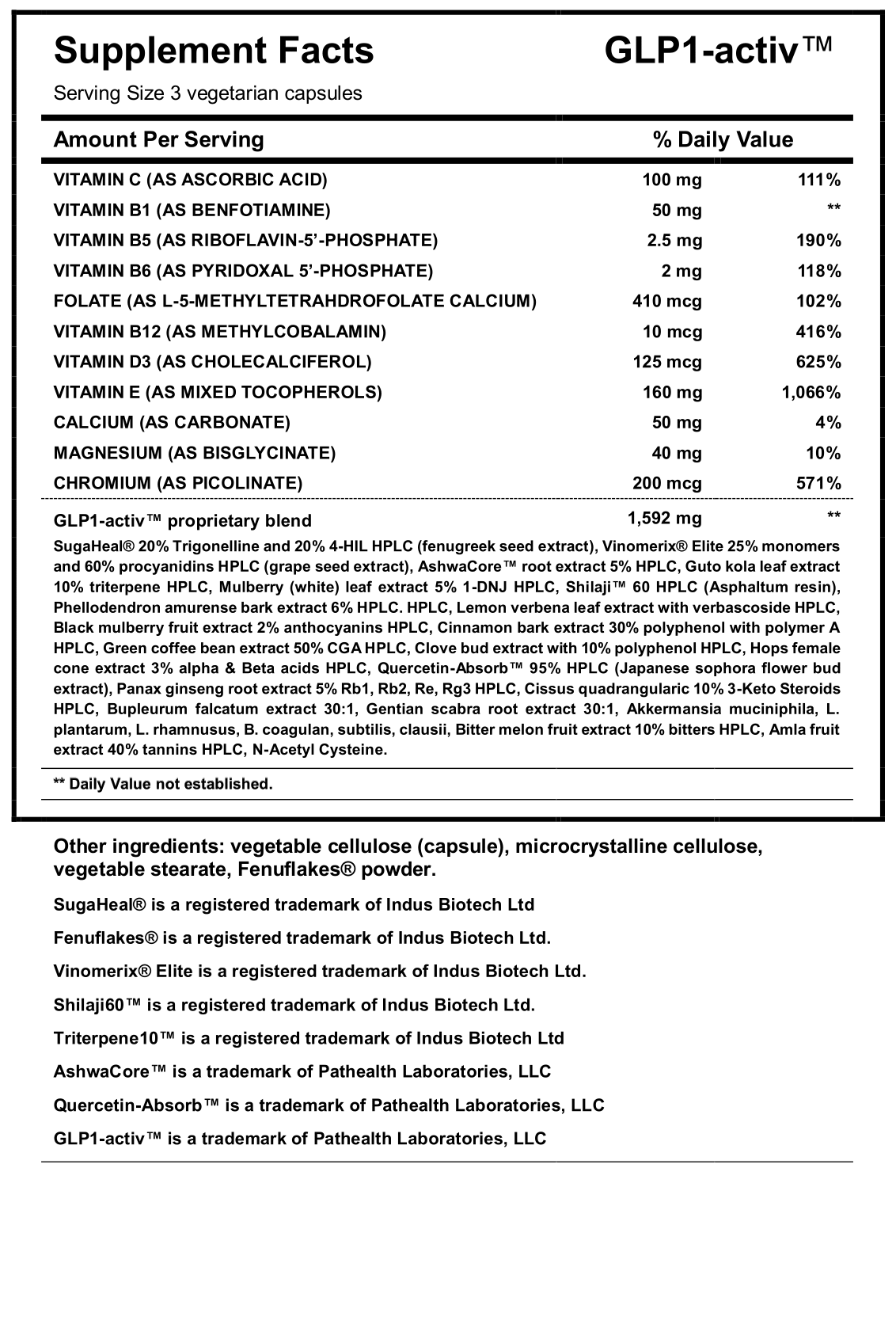
GLP1-activ
TM
Promotes healthy blood sugar, insulin, and lipid metabolism, as well as cardiovascular health*. May help support normal GLP-1 secretion*.
GLP-1 agonists are a relatively new class of drugs. They bind to and activate a cellular receptor for the hormone GLP-1 (glucagon-like peptide-1).
This cell receptor is most abundant in the insulin-secreting part of the pancreas. It is also present in the nervous system, and throughout the gastrointestinal tract, as well as the cardiovascular system, kidneys, and lungs.14,15
The formal name of this drug class is GLP-1 receptor agonists, but in common usage this has been shortened to GLP-1 agonist. These drugs act on the GLP-1 hormone receptor.
First developed as anti-diabetes medications, in the pancreas these drugs stimulate production of insulin, the hormone that helps reduce blood glucose levels after a meal.1,11
They also slow down the emptying of the stomach after eating and promote a feeling of fullness or satiety.11
Multiple meta-analyses of randomized controlled clinical trials have firmly established that GLP-1 agonist drugs are highly effective in type II diabetics for reducing blood sugar as well as hemoglobin A1C, a marker of longer-term glucose control. Some of these studies also found that these medications reduce systolic blood pressure.2,3,5
What has received so much attention is that these and other studies have also found that patients taking this class of drugs have had significant weight loss.
In part, this is because GLP-1 agonists activate receptors in the area of the brain that controls hunger.1,11,12 They stimulate satiety, the sense of feeling full after a meal, reducing cravings and caloric intake.GLP-1 agonists are approved for use in some people with type II diabetes, and two of them are FDA-approved for weight loss in certain people and situations.
In such individuals starting a GLP-1 agonist drug, it is recommended to also adopt a reduced-calorie meal plan and to increase physical activity at the same time.
Impressive Clinical Results
GLP-1 agonists have been found to offer benefit for a variety of common chronic conditions. Here are a few highlights:
Type II Diabetes
Meta-analyses of placebo-controlled trials of GLP-1 agonists in patients with type II diabetes2,3,5 have consistently shown that they are effective at reducing blood glucose.2-5
A hemoglobin A1c (HbA1c) test shows the average blood sugar level over two to three months. This value is higher in those with poor glucose control. In many clinical studies, use of a GLP-1 agonist has resulted in significantly lower HbA1c levels.
Weight Loss
The meta-analyses of randomized controlled trials in type II diabetics referenced above also found that, on average, subjects lost significant weight while taking these medications.2,3,5
In a trial of non-diabetic adults with obesity,7 all patients received a lifestyle intervention and were randomized to receive either weekly injections of semaglutide—the drug in Ozempic® and Wegovy® — or placebo. The semaglutide group experienced an average of nearly 15% reduction in body weight after 68 weeks, compared to 2.4% in a placebo group.
This corresponds to an average loss of almost 34 pounds in the treatment group, compared to less than six pounds in those who took a placebo.
Reduction in Cardiovascular Events
Both diabetes and obesity are risk factors for cardiovascular disease, which is damaging to both the heart and blood vessels. Rates of cardiovascular disease are much higher in those with poorly controlled diabetes and/or excess body weight. It makes sense that by controlling blood glucose and reducing weight, GLP-1 agonists could also lower cardiovascular risk.
Recent analyses have started to look at these effects and here too the results are encouraging. A meta-analysis of randomized controlled trials that included over 56,000 subjects taking GLP-1 agonists for diabetes found that the drugs reduced major cardiovascular events (including stroke and heart attack) and death from cardiovascular and all causes by 12%.7
Two trials 6,8 designed specifically to test cardiovascular effects of these drugs found that type II diabetics treated with semaglutide had a remarkable 21% and 26% reduction in risk for major cardiovascular events, including non-fatal stroke and heart attack, and death from cardiovascular causes.
- Available at: https://www.keckmedicine.org/blog/ozempic-for-weight-loss-los-angeles/. Accessed August 15, 2023.
- Andreadis P, Karagiannis T, Malandris K, et al. Semaglutide for type 2 diabetes mellitus: A systematic review and meta-analysis. Diabetes Obes Metab. 2018 Sep;20(9):2255-63.
- Avgerinos I, Michailidis T, Liakos A, et al. Oral semaglutide for type 2 diabetes: A systematic review and meta-analysis. Diabetes Obes Metab. 2020 Mar;22(3):335-45.
- Holmes P, Bell HE, Bozkurt K, et al. Real-World Use of Once-Weekly Semaglutide in Type 2 Diabetes: Results from the SURE UK Multicentre, Prospective, Observational Study. Diabetes Ther. 2021 Nov;12(11):2891-905.
- Li A, Su X, Hu S, Wang Y. Efficacy and safety of oral semaglutide in type 2 diabetes mellitus: A systematic review and meta-analysis. Diabetes Res Clin Pract. 2023 Apr;198:110605.
- Husain M, Birkenfeld AL, Donsmark M, et al. Oral Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N Engl J Med. 2019 Aug 29;381(9):841-51.
- Kristensen SL, Rorth R, Jhund PS, et al. Cardiovascular, mortality, and kidney outcomes with GLP-1 receptor agonists in patients with type 2 diabetes: a systematic review and meta-analysis of cardiovascular outcome trials. Lancet Diabetes Endocrinol. 2019 Oct;7(10):776-85.
- Marso SP, Bain SC, Consoli A, et al. Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N Engl J Med. 2016 Nov 10;375(19):1834-44.
- Zhao X, Wang M, Wen Z, et al. GLP-1 Receptor Agonists: Beyond Their Pancreatic Effects. Front Endocrinol (Lausanne). 2021;12:721135.
- Tachibana T. Glucagon-like peptide-1. In: Ando H, Ukena K, Nagata S, editors. Handbook of Hormones. San Diego: Academic Press; 2021:239-41.
- Cornell S. A review of GLP-1 receptor agonists in type 2 diabetes: A focus on the mechanism of action of once-weekly agents. J Clin Pharm Ther. 2020 Sep;45 Suppl 1(Suppl 1):17-27.
- Shah M, Vella A. Effects of GLP-1 on appetite and weight. Rev Endocr Metab Disord. 2014 Sep;15(3):181-7.
- Wilding JPH, Batterham RL, Calanna S, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. N Engl J Med. 2021Mar 18;384(11):989-1002.
- Cao C, Yang S, Zhou Z. GLP-1 receptor agonists and pancreatic safety concerns in type 2 diabetic patients: data from cardiovascular outcome trials. 2020 Jun;68(3):518-25.
- Lee J, Kim R, Kim MH, et al. Weight loss and side-effects of liraglutide and lixisenatide in obesity and type 2 diabetes mellitus. Prim Care Diabetes. 2023Oct;17(5):460-5.
Dietary polyphenols and the prevention of diseases.
Polyphenols are the most abundant antioxidants in the diet and are widespread constituents of fruits, vegetables, cereals, dry legumes, chocolate, and beverages, such as tea, coffee, or wine. Experimental studies on animals or cultured human cell lines support a role of polyphenols in the prevention of cardiovascular diseases, cancers, neurodegenerative diseases, diabetes, or osteoporosis. However, it is very difficult to predict from these results the effects of polyphenol intake on disease prevention in humans. One of the reasons is that these studies have often been conducted at doses or concentrations far beyond those documented in humans. The few clinical studies on biomarkers of oxidative stress, cardiovascular disease risk factors, and tumor or bone resorption biomarkers have often led to contradictory results. Epidemiological studies have repeatedly shown an inverse association between the risk of myocardial infarction and the consumption of tea and wine or the intake level of some particular flavonoids, but no clear associations have been found between cancer risk and polyphenol consumption. More human studies are needed to provide clear evidence of their health protective effects and to better evaluate the risks possibly resulting from too high a polyphenol consumption.
Crit Rev Food Sci Nutr. 2005;45(4):287-306
Isolation and characterization of polyphenol type-A polymers from cinnamon with insulin-like biological activity.
The causes and control of type 2 diabetes mellitus are not clear, but there is strong evidence that dietary factors are involved in its regulation and prevention. We have shown that extracts from cinnamon enhance the activity of insulin. The objective of this study was to isolate and characterize insulin-enhancing complexes from cinnamon that may be involved in the alleviation or possible prevention and control of glucose intolerance and diabetes. Water-soluble polyphenol polymers from cinnamon that increase insulin-dependent in vitro glucose metabolism roughly 20-fold and display antioxidant activity were isolated and characterized by nuclear magnetic resonance and mass spectroscopy. The polymers were composed of monomeric units with a molecular mass of 288. Two trimers with a molecular mass of 864 and a tetramer with a mass of 1,152 were isolated. Their protonated molecular masses indicated that they are A type doubly linked procyanidin oligomers of the catechins and/or epicatechins.
These polyphenolic polymers found in cinnamon may function as antioxidants, potentiate insulin action, and may be beneficial in the control of glucose intolerance and diabetes.
J Agric Food Chem. 2004 Jan 14;52(1):65-70
Green coffee bean extract improves human vasoreactivity.
Our previous study revealed the antihypertensive effects of green coffee bean extract (GCE) ingestion in spontaneously hypertensive rats. We suggested that this antihypertensive action was due to the fact that GCE contains chlorogenic acid (CQA) as a major phenolic compound, and CQA in turn contains ferulic acid as a metabolic component that acts on nitric oxide (NO) derived from the vascular endothelium. In this study, the effects of GCE on blood vessels were evaluated in healthy males. The subjects were 20 healthy males with reduced vasodilation responses measured by strain gauge plethysmograms (SPG) to ischemic reactive hyperemia. Of the 20 subjects, 10 (mean age, 37.2 years) ingested a test drink containing GCE (CQA: 140 mg/day), and the other 10 (mean age, 34.8 years) ingested a placebo drink for 4 months. During the ingestion period, SPG, pulse wave velocity (PWV), and serum biochemical parameters were measured, and acceleration plethysmograms (APG) were taken. The reactive hyperemia ratio (RHR) in the test drink group began to increase after ingestion for 1 month and was significantly higher (p <0.05) than that in the placebo group after ingestion for 3 months and 4 months. In addition, after ingestion for 4 months, the test drink group showed a significant decrease (p <0.01) in the plasma total homocysteine level compared with the pre-ingestion level. However, there were no significant differences in PWV or APG between the test drink group and the placebo drink group. The improvement in RHR after ingestion of a drink containing GCE suggested an improvement in vasoreactivity by this component.
Hypertens Res. 2004 Oct;27(10):731-7
A chlorogenic acid-induced increase in GLP-1 production may mediate the impact of heavy coffee consumption on diabetes risk.
Recent prospective epidemiology links heavy coffee consumption to a substantial reduction in risk for type 2 diabetes. Yet there is no evidence that coffee improves insulin sensitivity and, at least in acute studies, caffeine has a negative impact in this regard. Thus, it is reasonable to suspect that coffee influences the risk for beta cell “failure” that precipitates diabetes in subjects who are already insulin resistant. Indeed, there is recent evidence that coffee increases production of the incretin hormone glucagon-like peptide-1 (GLP-1), possibly owing to an inhibitory effect of chlorogenic acid (CGA — the chief polyphenol in coffee) on glucose absorption. GLP-1 acts on beta cells, via cAMP-dependent mechanisms, to promote the synthesis and activity of the transcription factor IDX-1, crucial for maintaining the responsiveness of beta cells to an increase in plasma glucose. Conversely, the “glucolipotoxicity” thought to initiate and sustain beta cell dysfunction in diabetics can suppress expression of this transcription factor. The increased production of GLP-1 associated with
frequent coffee consumption could thus be expected to counteract the adverse impact of chronic free fatty acid overexposure on beta cell function in overweight insulin resistant subjects. CGA’s putative impact on glucose absorption may reflect the ability of this compound to inhibit glucose-6-phosphate translocase 1, now known to play a role in intestinal glucose transport. Delayed glucose absorption may itself protect beta cells by limiting postprandial hyperglycemia — though, owing to countervailing effects of caffeine on plasma glucose, and a paucity of relevant research studies, it is still unclear whether coffee ingestion blunts the postprandial rise in plasma glucose. More generally, diets high in “lente carbohydrate”, or administration of nutraceuticals/pharmaceuticals which slow the absorption of dietary carbohydrate, should help preserve efficient beta cell function by boosting GLP-1 production, as well as by blunting the glucotoxic impact of postprandial hyperglycemia on beta cell function.
Med Hypotheses. 2005;64(4):848-53
The metabolic syndrome.
The metabolic syndrome is a common metabolic disorder that results from the increasing prevalence of obesity. The disorder is defined in various ways, but in the near future a new definition(s) will be applicable worldwide. The pathophysiology seems to be largely attributable to insulin resistance with excessive flux of fatty acids implicated. A proinflammatory state probably contributes to the syndrome. The increased risk for type 2 diabetes and cardiovascular disease demands therapeutic attention for those at high risk. The fundamental approach is weight reduction and increased physical activity; however, drug treatment could be appropriate for diabetes and cardiovascular disease risk reduction.
Lancet. 2005 Apr 16-22;365(9468):1415-28
Vitamins for chronic disease prevention in adults: scientific review.
CONTEXT: Although vitamin deficiency is encountered infrequently in developed countries, inadequate intake of several vitamins is associated with chronic disease. OBJECTIVE: To review the clinically important vitamins with regard to their biological effects, food sources, deficiency syndromes, potential for toxicity, and relationship to chronic disease. DATA SOURCES AND STUDY SELECTION: We searched MEDLINE for English-language articles about vitamins in relation to chronic diseases and their references published from 1966 through January 11, 2002. DATA EXTRACTION: We reviewed articles jointly for the most clinically important information, emphasizing randomized trials where available. DATA SYNTHESIS: Our review of 9 vitamins showed that elderly people, vegans, alcohol-dependent individuals, and patients with malabsorption are at higher risk of inadequate intake or absorption of several vitamins. Excessive doses of vitamin A during early pregnancy and fat-soluble vitamins taken anytime may result in adverse outcomes. Inadequate folate status is associated with neural tube defect and some cancers. Folate and vitamins B(6) and B(12) are required for homocysteine metabolism and are associated with coronary heart disease risk. Vitamin E and lycopene may decrease the risk of prostate cancer. Vitamin D is associated with decreased occurrence of fractures when taken with calcium. CONCLUSIONS: Some groups of patients are at higher risk
for vitamin deficiency and suboptimal vitamin status. Many physicians may be unaware of common food sources of vitamins or unsure which vitamins they should recommend for their patients. Vitamin excess is possible with supplementation, particularly for fat-soluble vitamins. Inadequate intake of several vitamins has been linked to chronic diseases, including coronary heart disease, cancer, and osteoporosis
JAMA. 2002 Jun 19;287(23):3116-26